Collarbone fracture rehabilitation in a Pilates studio setting
The collarbone is an area of the body that is commonly fractured in falls. Collarbone fractures can result from simple activities such as falling off our bicycle, playing tennis, skateboarding, skiing, playing touch football, car accident, or even an accidental trip after a few drinks! This article is about collarbone fracture rehabilitation, of particular relevance for a pilates studio setting:
- A review of the anatomy of the clavicle, also known as a collar bone;
- How the collar bone is commonly injured;
- What the healing process is for repair;
- What the safe and appropriate exercises are for a collar bone fracture.
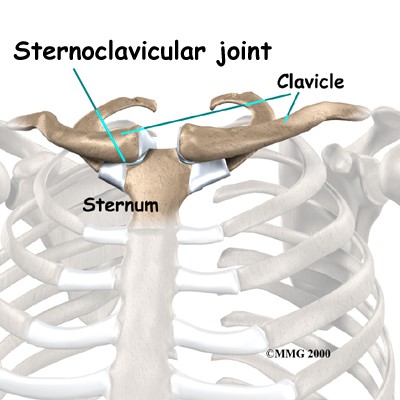
An anatomy review of the clavicle
The clavicle is a ‘lazy S’ shaped bone that is not fully ossified (becomes adult bone) until we are around 25 years of age. Due to this late maturation and generally higher levels of activity, young people are at a higher risk of fracture. Similarly due to structural degeneration and a higher risk of falls, fracture risk is also high in the elderly population and particularly in women.
The clavicle is important in that it attaches the shoulder girdle to the sternum, providing a strut or anchor point for the shoulder to articulate with the axial skeleton. Its other significant role is that it allows us to further extend movement of the scapula and thereby the arm away from the body. To understand how the arm and clavicle interrelate, put two fingers of your right hand on top of your left clavicle and gently pull down and away from your head. Now try and lift your left arm, note how it can be more difficult to lift that arm when the clavicle is not moving. The major muscles associated with movement of the clavicle and the shoulder include:
- Deltoids (anterior)
- Pectoralis major (clavicular head)
- Pectoralis minor (acts on scapula)
- Trapezius (upper fibres)
- Latisimus dorsi
The clavicle is also a major attachment site for the muscles of your neck, e.g. sternocleidomastoid and platysma muscles.

Focus on breathing work
A focus on breathing is also very important whenever we discuss the collarbone. A lot of muscles involved in breathing attach to the collarbone and if they are affected so to will the person’s breathing patterns and thoracic mobility. The anatomy and some ideas that can be added to collarbone work discussed in this article can be reviewed in our article on Thoracic Spine Exercises.
Most common site for collarbone fractures
The middle 1/3 of the collarbone is the most common site of fracture (~70% prevalence of collar bone factures), particularly in children. Medial fractures are uncommon (~3%), distal is more common (~28%) and has a higher occurrence rate in older people. A displaced fracture is when the bones after the injury have not aligned. Displaced fractures are more common in adults, likely due to the high-energy nature of the trauma e.g. car accidents. In the senior population this injury is more likely to occur from a fall directly onto the shoulder.
Common mechanisms of injury are a fall on the shoulder (lateral force) common in bicycle, football and skateboard injuries. When a person falls and fractures their collarbone they may also to have torn ligaments, particularly if the fracture occurs in the medial or lateral 1/3 as this is where the ligaments attach. This can have implications on healing and recovery time, and ongoing stability in the associated joint.
What is the repair process?
Bone fractures
Healing can best occur once the fracture is stable, which generally means immobilisation of those bones. There are many stages to the bone healing, which can take up to 2 years. The primary healing of bone typically occurs in 4-6 weeks, with remodelling and stronger secondary union taking approximately 12 weeks. During the remodelling stage between primary and secondary healing, the bony callus that has formed is still vulnerable to re-fracture or mal-union. To avoid this, weight bearing and lifting loads through the associated limb should be closely monitored and gradually progressed.
Ligaments
Ligamentous healing differs to that of bone in several ways. The healing time frame for a torn ligament is significantly longer relative to bone, and in the case of significant or full tears the strength and elastic properties of the ligament will not return to pre-injury state. Whilst this may sound worrying, it simply means that your body will need to adapt a more active strategy in stabilising these structures. It is important to de-load the ligaments during the first 2-4 weeks, to prevent re-rupture and allow the ligament to regain some elasticity. The most recent evidence indicates that guided return to loading is also extremely important, with gradual low load mobilisation from as early as one week following injury.
The introduction of low load work and range of motion movements should be progressed with supervision over the next 3 months, as the ligament fully heals and begins to remodel best with ongoing controlled loading much the same as bone.
Ligaments have a limited blood supply, therefore the remodelling process can take months and up to a year to reach maximal recovery. As a result rehabilitation and stabilisation of the bones will take time and ongoing management and appropriate progression.
What do you do when dealing with a collarbone fracture?
When you have a collarbone fracture to work with our starting point is that:
- Be aware of the injury site, the person could still do leg work when at the studio but it is probably not a good idea to lay the person on their side during early stages of a collar bone fracture recovery.
- Know what stage the person is at and that there will be a certain focus on the exercises for the arm and shoulder during that period of time. The person’s physiotherapist should have given them some exercises focusing on isometric strength, range of motion and then more global strength. When working with the clients it is important to help them focus on correct alignment and activation of the appropriate muscles. This will ensure that they are doing their homework correctly.
We have broken down the phases of collarbone fracture focus based on standard healing times for bones and ligaments. Understanding these healing times allows you to understand the structure’s capacity for load and movement. It is also important to remember that the bone structure is different for children, young adults and older adults and that this affects some of the healing and management process for these fractures.
Exercises for collarbone fracture rehabilitation
Early stages: Weeks 1-4
Immediately after the injury the collarbone must go through an inflammation and the start of tissue repair. Accordingly, immobilisation is important for the first 3-4 weeks to de-load bone and ligament as they begin to heal. A doctor and physiotherapist will generally recommend a splint of some type.
Children under 11 years old with non-displaced fractures do not usually require follow-up by a doctor or fracture clinic, assuming pain is remitting and there is no further displacement of the fracture as inflammation subsides and they are weened out of the sling. Children older than 11 years and adults will typically require follow-up with a doctor.
Mobilisation out of the sling commences at two weeks depending on pain control and if the fracture shows no sign of further displacement, with specific movements prescribed by the physiotherapist.
Daily exercise
To ensure optimal healing and to maintain strength, stability and mobility in surrounding structures, it is important to commence specific exercises in the first few weeks after injury.
The primary focus will be isometric strength and low-load or gravity minimised range of motion exercises, as prescribed by your physiotherapist. These may include: upper limb pendular movements; isometric shoulder movements; rotator cuff stabilisation.
The best approach is to be consistent and commit a small amount of each day to movement and exercises. Some exercises that could be included at this stage are:
- Pendulum exercises for the shoulders.
- Elbow/wrist range of motion exercises: elbow flexion/extension, forearm pro/supination; wrist flexion/extension; radial/ulnar deviation.
- Isometric holds of biceps/triceps/rotator cuff e.g. holds against wall, see rotator cuff video below.
Weeks 4-8: Range of motion and strengthening exercises
During this period of time the bone is starting to remodel and in reality this process can take years to complete, but the 8 week stage is a significant point in the remodelling process because of callus formation.
Children should be checked by their doctor if pain is increasing, or sensation changes abruptly. Sports and activities with physical contact should be avoided for the 8-12 weeks after the sling has been removed. A lump usually develops at the fracture site, which may be visible and palpable for months to years and is not cause for concern unless accompanied by significant swelling, pain or redness.
A physiotherapist will continue treating the soft tissue injuries and identify structural imbalances caused by a clavicle fracture. In addition, the physiotherapist will provide some specific exercises to gradually progress shoulder, elbow and wrist range of motion that you can work on in a pilates studio setting. These exercises can be added to other work with in the studio setting, within the guidelines set by the physiotherapist.
If the person is healing well, there should be a gradual increase in the range of motion exercises and they can begin strengthening exercises.
Exercises for Weeks 4-8
- Supported shoulder range of motion (ROM) exercises e.g. wall walk to comfortable ROM, see video seated knee stretch, seated wall ball roll.
- Wrist, elbow and hand ROM coupled movements e.g. biceps flexion with forearm supination or pronation, e.g. Incy Wincy Spider in the video below.
- Continued isometric work, e.g. the wall knee stretch in the video below.

Theraband neck exercise is another good isometric exercise to add in at this stage, remembering that many neck muscles attach to the collar bone.

The deltoids attach to the clavicle. In injuries they can tighten in protection. These exercises with Makarlu Lotus are about triggering the muscle to relax it rather than stretching it.

Triggering through the triceps can help release their pull on the scapula. Remember that the scapula articulates with the collar bone.
Trigger through the bicep with Makarlu Lotus. In this position you can also achieve a nice pec release.
Weeks 8-12: Range of Motion exercises
During this period the focus will be on working toward a full range of motion in all directions. The strengthening exercise program will continue to progress, but heavy lifting should be avoided. Focus on rebuilding muscle endurance, with light resistance and higher repetitions. This gives bone and ligaments adequate loading to promote remodelling but should avoid over-stressing and causing delayed healing in these structures.
At this stage some of the exercises could include:
- Active ROM exercises e.g. Theraband rows, dowel passovers, Theraband rotator cuff, gradual return to full ROM in all directions of movement with good movement proficiency. Some videos below from the reformer repertoire can be useful.
- Isometric holds throughout ROM to build endurance.
- Shoulder stabilisation, e.g. incline or 4 point kneel shoulder taps, add Makarlu Lotus or ball to challenge.
- Some focused exercises from the pilates reformer repertoire, making sure that there is good movement practice applied.
Weeks 12-16: Strengthening exercises
By this stage a physiotherapist is likely to consider that a person will be ready to progress to increased strengthening work. As always, if there is a significant increase in pain, a sense of instability, or painful catches in a joint during movement, then stop and seek advice.
An example of exercises that could be introduced include:
- Loaded overhead movements e.g. shoulder press. Start with the bottom loaded supine push through bar work and then progress to an overhead press, see images below.
- Begin sports specific skill drills and exercises, e.g. passing, catching, throwing.
Return to specific sports training and competition only when you are cleared for activity and your functional testing shows that your injured side is as strong and mobile as the uninjured side. This is particularly important for high impact sports like football (Rugby, Gridiron, Australian Rules). If your client is not an athlete, and let’s face it the majority of collarbone injuries are in non-athletes, getting your body strong is an important priority for physical safety and confidence.
Some specific exercises during this period include:
- Progress ROM exercises, adding some resistance with Theraband, increased strength.
- Dynamic stability work, e.g. shoulder taps in plank, walk outs using CoreAlign or using the wunda chair as in the video below.
- Strength for scapula and rotator cuff, e.g. PTB press ups, see video below. Also if in a gym setting add in dumbbell shoulder press, reverse fly, overhead squats.
- Sport specific drills if applicable e.g. throwing/catching/passing or low impact contact drills, gradually increasing intensity over the next 8 weeks.

Caddie PTB press ups. Modify the load through the resistance of the spring, slowly progressing load. Once the person has achieved an overhead load clearance start to add in exercises like bottom loaded roll up.

In this series Max is working through plank and other shoulder girdle movements by using the Makarlu hardwood base as a slider to facilitate more dynamic movement.
Remember also that pilates is a life long mind body practice. A good pilates teacher provides individualised focus and adaptation, developing trust with their clients over long periods of time. During times of injuries it is understandable that the client wants to continue their practice and it is important to work in conjunction with the person’s manual therapist to ensure client safety and focus in performing specific exercises for recovery.
This article was written by Carla Mullins (Pilates teacher with Body Organics) and Lachlan Loose (physiotherapist with Body Organics).
Carla Mullins is Director of Education at Body Organics with many years experienced in Pilates, Gyrotonic, CoreAlign and other movement modalities. She is currently undertaking a Bachelor of Occupational Therapy at University of Queensland. Carla covers topics such as the collarbone, its movement and injury recovery in courses in Australia and the USA, such as Anatomy Dimensions Upper Limbs.
References
Hunter JB. Fractures around the shoulder and humerus. In Children’s Orthopaedics and Fractures,3rd Ed. Benson M, Fixsen J, Macnicol M, Parsch K (Eds). Springer, London 2010. p.717-30.
Lenza M, Belloti JC, Andriolo RB, Gomes Dos Santos JB, Faloppa F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst Rev 2009; CD007121.
Klein SM, Badman BL, Keating CJ, Devinney DS, Frankle MA, Mighell MA. Results of surgical treatment for unstable distal clavicular fractures. J Shoulder Elbow Surg 2010; 19: 1049-55.
Simon RR, Sherman SC, Koenigsknecht SJ. Clavicle fractures. In Emergency Orthopaedics – The Extremities. 5th Ed. McGraw-Hill, Chicago 2007. p.285-7.
Young SJ, Barnett PL, Oakley EA. Fractures and minor head injuries: Minor injuries in children II. Med J Aust 2005; 182: 644-8.
© 2018 Body Organics Pty Ltd. All Rights Reserved. Body Organics®, Makarlu®, Inspired by Nature. Designed for Movement.™, Anatomy Dimensions™ and HedgeHog™ are trade marks of Body Organics Pty Ltd. Makarlu Patent Pending.
Comments are closed.